what can cause a shoulder to jerk unexpectedly
What is Functional Jerks and Twitches (Myoclonus)?
Functional myoclonus refers to sudden jerky or shock like movements that occur every bit part of a functional movement disorder.
Myoclonus is a symptom institute in a broad range of neurological diseases as well equally some normal states.
Most people have had the experience of jumping or jerking as they are dropping off to sleep. These movements are chosen 'hypnic jerks'.
Most people are also familiar with the random trunk 'shudder' that some people get. This is sometimes described as 'walking on someones grave' because of the manner it moves quickly through the body.
The occasional hypnic wiggle or a body shudder are normal. Only in functional myoclonus the jerks become a frequent and disabling problem.
At that place may be jerks of the artillery or legs, or quite commonly at that place is jerking in the trunk. The movements cannot exist controlled (ie they are involuntary.
How does information technology begin?
Functional myoclonus ofttimes begins quite of a sudden (in effectually two thirds of cases) but may be gradual. Information technology affects patients somewhat later than some of other symptoms described on this website. For instance in i series of 35 patients the boilerplate age it started was 45. It may follow on from one of the following situations
- A physical injury. Functional myoclonus may occur equally part of complex regional pain syndrome. Jerks in the trunk commonly back-trail back pain.
- Later on experiencing myoclonus from a medical trouble such equally
a. a side effect of a medication
b. a faint with some hasty movements
c. an infection
d. a period of hospitalisation in intensive intendance - Afterwards having a "fright" or a panic attack
- With a symptom called 'dissociation' (spaced out or 'zoned out') which can happen without whatsoever feelings of fright.
- An underlying mild additional cause of myoclonus which has become 'amplified' because of functional myoclonus.
How is the diagnosis fabricated?
The diagnosis of functional myoclonus is normally made by a neurologist. Information technology can be hard diagnosis to make because it requires expert cognition of the full range of jumps and jerks due to neurological affliction, many of which are unusual .
The following are some examples of things a neurologist would await for to diagnose functional myoclonus
- Jerks of the torso (i.east.trunk) rather than the legs
- Sudden onset of the condition "out of the blue" with no other obvious disease cause
- Involvement of the face up and/or phonation in a patient who otherwise has bodily jerks
- Flexion jerks of the trunk when walking
- Jerks which can exist suppressed or delayed by the patient using distraction techniques
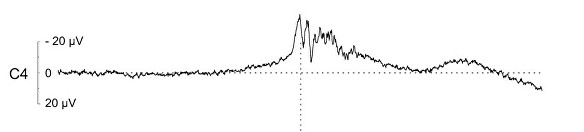
- In some research settings the patient can have an investigation called 'EEG jerk-locked back averaging'. This is to look for changes in the encephalon moving ridge (EEG) that typically precede the jerk in patients with functional myoclonus. This modify is called a Bereitschaftspotential (BP). You can only run across this if you tape lots of jerks in one individual. This is a difficult investigation to conduct out and is more than of a research tool than a routine examination. The movie below shows a BP in a patient with functional myoclonus
Over half of patients with functional myoclonus draw warning symptoms before some of their jerks. These may last merely seconds or sometimes minutes. Some patients draw a rising sense of tension which somehow the jerk gets rid of temporarily. And so they dont want to take the jerk but it is doing something useful, some of the time. Understanding this can be useful in treatment
If you don't get any warning then don't be put off by the paragraph above. It doesn't utilize to everyone with functional myoclonus.
What is the treatment?
Take a wait through the pages on treatment but here are some specific points.
Exercise you have confidence in the diagnosis?
It is essential that you feel that you have the correct diagnosis. If you don't it will be hard to put into practice the rehabilitation techniques suggested here.
If you don't feel that you have functional myoclonus you demand to expect at what basis the diagnosis has been fabricated. You should take some of the clinical features described above. If yous do, why don't you take confidence in the diagnosis yous accept been given?
You exercise non need to be stressed to accept functional myoclonus. In fact functional myoclonus is oft most noticeable when people are relaxed or not thinking near anything in particular. Peradventure yous rejected the diagnosis considering the doctor suggested it was "stress related"? – at that place may have been a misunderstanding if that was the example.
We know that many patients with functional myoclonus do have stress every bit a cause of their symptoms, just many don't. So whether you lot have been stressed or not is not relevant to the diagnosis.
Specific techniques
The handling of functional myoclonus is quite challenging. Normally the problem has been going on for some time and has go a 'addiction' that the brain has got in to. The following may be worth considering
- If you do get even the slightest warning stage so try to apply distraction techniques to see if yous tin avoid a wiggle. You can utilize the same techniques that are described for dissociative attacks. Some patients report that when they do this they tin can be successful but then accept a jerk or series of jerks that are even worse immediately afterwards. Merely keep trying – you may find it'south 1 way to 'intermission the addiction'.
- Are you expecting to have jerks at a certain time – for example when you prevarication downwardly at night to sleep or are in a public place. The mode the brain works means that sometimes if y'all really await something to happen, it will, even though you don't want it to. This is called a 'conditioned response' and is something that is well understood by psychologists when they retrieve virtually habits in the brain. If yous try to challenge those thoughts and then perhaps it can alter your jerks
- Medication -is oft disappointing in functional myoclonus. About patients have tried medicines like clonazepam without success
- Hypnosis – Sometimes under hypnosis, jumps and jerks may improve and you may be able to learn self hypnosis to practice at home
Unfortunately many patients with functional myoclonus find that it is a problem which persists. But its certainly worth trying to ameliorate it. Fifty-fifty knowing what it is tin can give people valuable peace of heed.
A note on Benign Muscle twitches – these are sometimes chosen 'beneficial fasciculations'.
Benign fasciculations are not usually considered a functional disorder, just they are benign, cause concern and may coexist with some of the other symptoms on this website which is why I mention them
Nearly people have small-scale twitches from fourth dimension to time, especially around the eye and in the fingers. Such twitching is and so mutual that to experience information technology occasionally is normal.
Notwithstanding, some people find that they experience more and more of this muscle twitching until it is present in multiple areas of their torso, for about of the time. This can lead to understandable anxiety nigh what is causing the symptoms, which in turn makes the twitching even worse.
Generalised benign twitching like this is known to occur more frequently in medical students and doctors who, on developing these symptoms, worry that they might take motor neurone disease (known in the USA every bit ALS).
In fact the twitching seen in this condition, which affects the whole musculus fibre, is dissimilar to the smaller wriggling movements, chosen fasciculations, seen in motor neurone disease. The condition is therefore somewhat misnamed every bit benign fasciculation. There are other causes of generalised muscle twitching but benign fasciculation remains the most common clinically.
Every bit with functional symptoms, knowing what the problem is tin can help it to settle spontaneously.
This is an article written by a medico who experienced benign fasciculations and health anxiety which later on resolved with treatment.
Source: https://www.neurosymptoms.org/en_GB/symptoms/fnd-symptoms/functional-jerks-and-twitches/
0 Response to "what can cause a shoulder to jerk unexpectedly"
Publicar un comentario